
Injury Induced by Chemical Warfare Agents
Injury Induced by Chemical Warfare Agents: Characterization and Treatment of Ocular Tissues Exposed to Nitrogen MustardInjury Induced by Chemical Warfare Agents: Characterization and Treatment of Ocular Tissues Exposed to Nitrogen Mustard
Eyal Banin,1 Yair Morad,2 Eduard Berenshtein,3 Alexey Obolensky,1 Claudia Yahalom,1 Jacob Goldich,3 Fatih M. Adibelli,1 Gladys Zuniga,1 Maribel DeAnda,1 Jacob Pe’er,1 and Mordechai Chevion3
PURPOSE. Mustard agents are highly toxic and abundant warfare chemicals, primarily affecting ocular tissues, with no specific treatment antidote. The purpose of the present study was to examine the efficacy of novel metallocomplexes, known to inhibit the formation of highly reactive free radicals, to reduce ocular injury induced by nitrogen mustard (NM).
METHODS. One eye in each of 72 rabbits was exposed to 1% to 2% NM. Topical treatment with eye drops of a metallocom-plex— either zinc- or gallium-desferrioxamine (Zn/DFO and Ga/DFO)—was compared with treatment with saline, zinc (chloride), or DFO alone. Examiners masked to the treatment groups assessed the extent of ocular injury and the response to treatment using clinical, histologic, and biochemical criteria.
RESULTS. Exposure to NM followed by administration of carrier alone (saline) caused severe and long-lasting injury to ocular anterior segment structures. Treatment with either Zn/DFO or Ga/DFO yielded marked protection (52%– 64%), including faster healing of corneal epithelial erosions, less scarring and neovascularization, decreased inflammation in the anterior chamber, better maintenance of intraocular pressure, and less severe changes in the iris and lens. These were also associated with better preservation of systemic antioxidant status. Zinc or DFO alone afforded lower levels of protection. No toxic effects of these complexes were observed.
CONCLUSIONS. It is suggested that Zn/DFO or Ga/DFO, by virtue of their enhanced ability to infiltrate cells and inhibit transition metal-dependent formation of free radicals through the com-bined push–pull mechanism, be considered as a basis for treat-ment of mustard injuries. (Invest Ophthalmol Vis Sci. 2003;44: 2966 –2972) DOI:10.1167/iovs.02-1164
Mustard agents are among the most powerful tactical chemical weapons that exist today. Sulfur mustard was first used in Ypres, Belguim, in World War I, and throughout
From the Departments of 1Ophthalmology and 3Cellular Biochem-istry and Human Genetics, Hebrew University-Hadassah Schools of Medicine and Dental Medicine, Jerusalem, Israel; and the 2Department of Ophthalmology, Assaf Harofeh Medical Center, Zrifin, Israel.
Supported by grants from the Israel Defense Forces Medical Corps and from the Pepka and Dr. Moshe Bergman Memorial Fund. MC is the incumbent of the Dr. William Ganz Chair of Heart Studies.
Submitted for publication November 15, 2002; revised January 10, 2003; accepted January 17, 2003.
Disclosure: E. Banin, None; Y. Morad, None; E. Berenshtein, None; A. Obolensky, None; C. Yahalom, None; J. Goldich, None; F.M. Adibelli, None; G. Zuniga, None; M. DeAnda, None; J. Pe’er, None; M. Chevion (P)
The publication costs of this article were defrayed in part by page charge payment. This article must therefore be marked “advertise-ment” in accordance with 18 U.S.C. §1734 solely to indicate this fact.
Corresponding author: Eyal Banin, Department of Ophthalmol-ogy, Hadassah-Hebrew University Hospital, P.O. Box 12000, Ein-Karem, Jerusalem 91120, Israel; banine@md.huji.ac.il.
the war, approximately 1,200,000 soldiers were exposed to it. Approximately one third of them required prolonged medical treatment for dermal, gastrointestinal, respiratory, and ocular injuries.1 More recently, mustard was used in the Iran–Iraq conflict against Kurdish civilians2 and Iranian troops.3 In view of the recent surge in international terror activity, the relative abundance of this weapon and the ease of its production and deployment raise the concern that it could be used by terror-ists, as well as on the battlefield.
Incapacitating short- and long-term ocular injuries are major manifestations of mustard toxicity, affecting up to 90% of those exposed. Approximately 10% of Iranian mustard casualties ex-hibited ocular injuries that persisted for several months, de-spite treatment. Indeed, reports of delayed keratopathy in veterans of this war have recently appeared.4
Generally, exposure to mustard agents produces eye inflam-mation to varying degrees. Although the toxic chemical reacts rapidly with ocular tissues after contact, discomfort and injury are usually delayed for hours. Symptoms begin with eye pain, photophobia, excessive tearing, and blurred vision. Physical findings include spasm of the eyelids, swelling and edema of skin and tissues around the eyes, conjunctival injection, and inflammation of the anterior chamber of the eye. The intraoc-ular pressure (IOP) may increase and remain elevated for a few days. After several hours, the corneal epithelium begins to form vesicles and slough. In severely injured eyes, there is constric-tion of the pupils, dilatation of blood vessels within the iris, hemorrhages, and necrosis. Chemical anterior uveitis develops, leading to adhesions of the iris to the lens capsule with ensuing cataract formation. Late sequelae include corneal scarring and neovascularization as well as severe and chronic elevation of IOP due to neovascular glaucoma.5,6
Strong evidence indicates that mustard injury is mediated, at least in part, by the formation and action of reactive oxygen species (ROS), in addition to its action as an alkylating agent. This notion is supported by the findings of a dramatic increase (30-fold) in copper levels7 and a decrease in ascorbic acid within the anterior chamber8 after ocular exposure to mustard compounds, both being indicators of oxidative stress. Free radicals have also been shown to play a role in corneal inflam-mation after exposure to other ocular irritants, such as alkali substances.9,10 In such cases, tissue damage after corrosive injury to the cornea is exacerbated by penetration of ROS to the corneal stroma, because they fragment DNA chains, poly-merize or depolymerize proteins and hyaluronate, and destroy lipid membranes.10 ROS, such as the superoxide anion, reduce ferric iron (Fe3 ) and copper (Cu2 ) and produce the highly reactive hydroxyl radicals, Fe2 and Cu . These reduced metal ions, in turn, can react with H2O2 to produce the hydroxyl radical, which causes further damage. If indeed the formation of ROS is part of the pathogenesis of mustard-induced injury, curbing their formation could be highly beneficial.
2966 Investigative Ophthalmology & Visual Science, July 2003, Vol. 44, No. 7 Copyright © Association for Research in Vision and Ophthalmology IOVS, July 2003, Vol. 44, No. 7 Effective Treatment of Mustard Injuries 2967TABLE 1. Experimental and Control Groups Group 1a 1b 2a 2b 3 4 5 6 NM(%)* 1 2 1 2 1 1 None 2 Treatment† Saline Saline Zn/DFO Zn/DFO ZnCl2 DFO Saline Ga/DFO Eyes (n) 12 8 12 8 12 12 8 8
* NM, nitrogen mustard concentration (wt/vol %).
† Treatment, the type of treatment drops used in each group; Saline, normal saline; Zn/DFO, zinc desferrioxamine, Ga/DFO, gallium desferrioxamine, both at a concentration of 3.5 mM; ZnCl2, zinc chloride (Aldrich Chemical Company, Inc., Milwaukee WI) at a concentration of 3.5 mM; DFO, Desferri-oxamine (Desferal; Ciba-Geigy LTD, Basel, Switzerland) at a concentration of 3.5 mM in saline; Zn/DFO and Ga/DFO were prepared by dissolving the chloride salt of the metal in doubly distilled water, maintaining pH at 3, and adding DFO at an equivalent concentration, followed by titration to pH 7.4 with sodium bicarbonate. The stock was diluted in saline to a final concentration of 3.5 mM, based on DFO concen-tration.
Zinc desferrioxamine (Zn/DFO) and gallium desferrioxam-ine (Ga/DFO) are novel metal complexes that inhibit the catal-ysis of iron (and copper) in the formation of free radicals. Their protective activity can be visualized through the “pulling” out of redox active iron that is responsible for the production of the hydroxyl radicals through chelation by the DFO compo-nent. At the same time, the relatively inert zinc (or gallium) ion that is liberated during the exchange of iron within the com-
plex, further acts as a secondary antioxidant, by “pushing” out additional iron ions from their catalytic binding sites.11,12 Thespatial structure of these complexes is markedly different from that of desferrioxamine alone, enhancing their ability to infil-trate cells and tissues.12 In previous studies, we have shown that systemic treatment with Zn/DFO and Ga/DFO reduces damage to the retina subjected to ischemia and reperfusion, in accord with their enhanced infiltration through the blood– retinal barrier.13,14 Similarly, topical application of Zn/DFO reduces corneal damage after alkali burn.15 We therefore sought to examine the effectiveness of topical application of Zn/DFO and Ga/DFO in reducing ocular damage after expo-sure to nitrogen mustard (NM).
METHODS
Treatment Groups and Protocol
The experimental and control groups are detailed in Table 1. They differ in concentration of NM applied and in the treatment drops used.Groups 1 and 5, as well as the fellow uninjured eye in each animal, served as the controls. In group 1, examining the effect of placebo (saline) drops on injured eyes effectively served as the model for exposed but not treated eyes. These were compared with groups 2, 3, 4, and 6. In group 5, normal saline was applied in the trephine (no exposure to mustard). In this group both eyes of each animal served as experimental eyes. In the other groups, in each animal, the fellow control eye served to assess the question of possible toxicity of the treatment drops used in that animal when the drops were applied to practically healthy eyes.
Immediately after exposure to NM, 2 drops of one of the different treatment medications listed in Table 1 were administered every hour for 12 hours in both experimental and control fellow eyes. From the second day onward, until the end of the experiment at 4 weeks, drops were given seven times daily (every 2 hours). Antibiotic ointment (chloramphenicol 5%) was applied every night to all eyes throughout the experiment. Application of the drops was performed in a blind fashion with caregivers masked to the content of the bottles of medication.
Animal Model of Ocular NM Injury
Seventy-six New Zealand Albino rabbits weighing 2.5 to 3.5 kg were used. All animal experiments were conducted in compliance with the ARVO Statement for the Use of Animals in Ophthalmic and Vision Research. Animals were anesthetized with ketamine HCl (50 mg/kg) injected intramuscularly in combination with the relaxing agent xyla-zine (5.0
mg/kg). Local anesthetic drops (benoxinate HCl 0.4%; Fischer Pharmaceuticals, Tel-Aviv, Israel) were administered. To induce ocular mustard injury, NM (mechlorethamine) at a concentration of 1% wt/vol (48 rabbits) or 2% wt/vol (24 rabbits) was applied to the cornea of one eye of each animal (the experimental eye) for 5 minutes within a trephine. The vacuum trephine was used to limit the area of applica-tion to a circle 4 mm in diameter in the center of the cornea. Imme-diately after application, NM was quickly absorbed from within the trephine, with small sponges (Weck-Cel; Medtronicsolan, Jacksonville, FL), followed by washing of the eye within the trephine with copious amounts of normal saline. The trephine was then removed, and the eye was again washed intensively with additional normal saline. Local treatment was immediately initiated according to the protocol de-scribed below. In control eyes (four additional animals, eight eyes), saline solution (instead of NM) was applied to the cornea for 5 minutes within the trephine. In control treatment, the vehicle (saline) was used as eye drops after exposure to NM. During the experiment and follow-up, intramuscular dipyrone injections (10 mg/kg) were given to ani-mals showing pain or distress. This was necessary mainly during the first 5 to 10 days after injury.
Follow-up Parameters
Magnitude of ocular injury and response to treatment were assessed by examiners masked to the treatment groups. Repeated slit lamp exam-inations with scoring of anterior segment injury, measurements of IOP, color photographs of the anterior segment, fluorescein angiography (FA), electroretinography (ERG), and blood testing of antioxidant sta-tus were performed according to the following timetable and guide-lines.
Slit Lamp Examinations. These were performed at 24 hours after injury and then repeated at 3, 7, 14, 21, and 28 days. In each examination, the following parameters were recorded:
1. Area of corneal epithelial loss (corneal erosion): The average horizontal and vertical linear dimensions of the epithelial defect
as stained by locally applied fluorescein were measured using the adjustable slit lamp beam and the area computed in mm2.
2. Degree of corneal opacity: grade 0, clear cornea with iris details seen clearly; grade 1, mild blurring of iris details; grade 2, moderate opacity with blurred iris crypts; and grade 3, severe corneal opacity, no iris details seen.
3. Degree of iris pigmentation: grade 0, no pigmentation; grade 1, mild; grade 2, moderate; and grade 3, severe iris pigmentation.
4. Additional observations recorded included extent of eyelid and conjunctival swelling and injection; anterior chamber reaction; and, when present, hyphema, corneal ectasia, perforation, and resultant endophthalmitis. 2968 Banin et al. IOVS, July 2003, Vol. 44, No. 7

FIGURE 1. Corneal and conjunctival injury in eyes 4 weeks after ex-posure to 2% NM. (A–C) Slit lamp photographs of the anterior seg-ment. Note marked conjunctival edema and hemorrhages (A) and corneal neovascularization and opacity (B) in saline-treated eyes. In eyes treated with Ga/DFO (C) changes were much less severe. (D–F) Corneal histology. In contrast to the normal cornea in a nonexposed rabbit eye (D), acanthosis, irregularities and some keratinization of the corneal epithelium, and infiltration of the corneal stroma with inflam-matory cells, blood vessels, and hemorrhages was seen in a NM-exposed, saline-treated eye (E). There was also lysis of the extracellular matrix in the superficial stroma (E). Markedly milder changes occurred in the NM-exposed, Ga/DFO-treated eye (F).
Intraocular Pressure. Repeated IOP measurements were per-formed in eight eyes each from the following groups: group 1b (2%NM saline), group 2b (2%NM Zn/DFO), group 6 (2%NM Ga/ DFO), and group 5 (saline “injury”). Baseline IOP was measured before NM (or saline) exposure and remeasured on days 1, 3, 7, 10, 14, 21, and 28 after injury. A handheld automated tonometer (Tonopen; Men-tor, Norwell, MA) was used.
Color Photographs and FA. Color photographs of the ante-rior segment and iris FA were performed at 28 to 35 days after injury using a modified fundus camera (CF-60UV; Canon, Tokyo, Japan). These were used to grade corneal opacity and iris involvement by three additional independent and masked observers at this time point.
Electroretinography. To examine possible involvement of the posterior segment in NM-induced injury, as well as possible toxic-ity of the Zn/DFO complex in itself, retinal function was assessed by performing ERG recordings in four animals from groups 1 and 2 at 6 to 7 weeks after injury. Pupils were dilated with 1% tropic-amide and 2.5% phenylephrine. Anesthetized animals were dark adapted for at least 60 minutes. After application of local anesthetic drops, a Burian-Allen contact lens electrode was inserted in both eyes with a clip electrode placed on one ear serving as a ground. The dark-adapted (DA) rod response, dark-adapted mixed cone-rod response, and light-adapted (LA) 1- and 30-Hz cone responses were recorded according to International Society for Clinical Electro-physiology of Vision (ISCEV) standards with a computerized ERG system and a Ganzfeld bowl (UTAS 3000; LKC Instruments, Gaithers-burg, MD). All ERG responses were filtered at 0.3 to 500 Hz, and signal
TABLE 2. Area of Corneal Epithelial Damage after Exposure to 1% NM
Days Experimental Groups after Exposure Zn/DFO Saline ZnCl2 DFO 1 28.3 6.4 32.0 4.5 36.0 2.9 28.5 6.33 11.2 3.9* 28.3 3.2 23.3 4.6 24.3 4.7
Data are expressed in square millimeters (mean SEM). n 6 for each group.
* Corneal epithelial erosion in Zn/DFO-treated eyes was signifi-cantly smaller than in saline treated eyes at 3 days after exposure (P 0.05; Mann-Whitney test).
FIGURE 2. Degree of corneal opacity after exposure to 1% NM. Initial injury and opacity were similar among the different experimental groups one day after injury. However, 4 weeks later, corneal opacity was markedly reduced in Zn/DFO- and DFO-treated eyes compared with saline-treated eyes (*P 0.05, Pearson 2 test). Eyes treated with ZnCl2 showed a similar trend. Observers who were masked to the treatment regimen performed grading of corneal opacity according to a four-point severity scale. Data in each bar represent mean score of six eyes.
averaging was used. The fellow (uninjured) eye in each animal served as the control.
Systemic Antioxidant Status. Ascorbic acid (AA), a naturally occurring free radical scavenger, is normally present in blood. At 1, 7, 14, and 28 days after injury, blood samples were obtained, and systemic oxidative stress was assessed by measurement of AA dissipation. AA, the reduced form of ascorbate and the fraction of the oxidized ascorbate (dehydro-ascorbate, DHAA) were measured,16 and the ratio between them was calculated and denoted as OSAA (see equation in Fig. 8).17
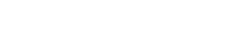
FIGURE 3. Degree of iris pigmentation 4 to 5 weeks after exposure to 1% NM. (A–C) Areas of iris pigmentation as well as areas of atrophy were seen in NM-exposed, saline-treated eyes (A) that were not present in noninjured fellow eyes (B) and were markedly reduced in NM-exposed, Zn/DFO-treated eyes (C). (D) Mean iris pigmentation score at 4 to 5 weeks after injury was significantly reduced in Zn/DFO-treated compared with saline-treated eyes, representing a 64% protec-tive effect (*P 0.05, Pearson 2 test). Treatment with each compo-nent of the complex separately (ZnCl2 or DFO) showed a trend for reduction in severity. Observers masked to the treatment regimen performed grading of iris pigmentation according to a four-point se-verity scale. Data represent mean score of six eyes. IOVS, July 2003, Vol. 44, No. 7 Effective Treatment of Mustard Injuries 2969
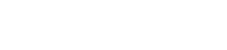
FIGURE 4. Iris FA at 4 to 5 weeks after exposure to 1% NM shows that iris pigmentation and atrophy differed among the treatment groups. In-tegrity of iris vessels was not compromised, and no leakage had occurred at that time. (A) Control (no exposure to NM); (B) 1% NM saline; (C) 1% NM Zn/DFO; (D) 1% NM ZnCl2; (E) 1% NM DFO.
Histology of Ocular Structures
At 4 to 8 weeks after NM injury, eyes of two to four animals from each group were obtained for histologic examination. Eyes were enucleated and fixed in 4% paraformaldehyde. After specimens were embedded in paraffin, 4- m sections were cut and stained with hematoxylin and eosin for histologic evaluation of injury. In a number of eyes, Prussian blue staining was performed to identify hemosiderin.
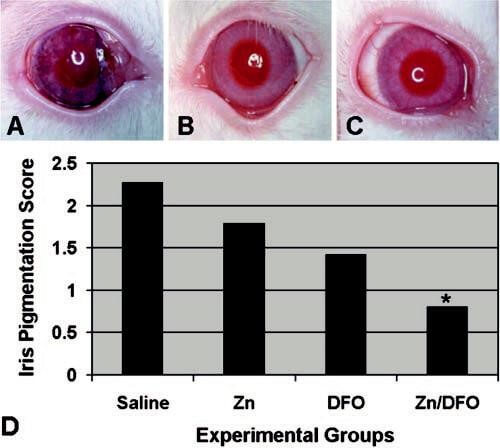
FIGURE 5. Prussian blue staining showed the presence of hemosiderin in anterior segment structures of eyes 4 weeks after exposure to 2% NM. (A) 2% NM saline; (B) 2% NM Ga/DFO; (C) 2% NM saline; (D) 2%NM Ga/DFO. Note markedly reduced ferritin and hemosiderin staining in Ga/DFO-treated eye compared with saline-treated. Magnifi-cation: (A, B) 10; (C, D) 50.
FIGURE 6. Iris and lens injury 4 weeks after exposure to NM. (A–C) Nonexposed, control eye; (D–F) 2% NM, saline-treated eye; (G–I) 2% NM, Ga/DFO-treated eye. Note that loss of the normal iris protrusions (rugae) and inflammatory cell infiltration in NM-exposed eyes was more severe in the saline-treated (D) than in Zn/DFO-treated (G) eye, compared with the nonexposed eye (A). Adhesions of the iris to the lens occurred in the saline-treated eye (E) but not in the control (B) or Zn/DFO-treated (H) eyes. Cataractous lens changes including epithelial necrosis and formation of morgagnian globules was also more severe in the saline-treated (E, F) than in Zn/DFO-treated (I) eyes.
2970 Banin et al.
Statistical Evaluation
Gradable parameters were averaged in each treatment group at the different time points. The Mann-Whitney test was used for comparison of parametric data (i.e., erosion area, IOP, OSAA), and the Pearson 2 test was used for comparison of nonparametric data (i.e., degree of corneal opacity or degree of iris pigmentation).
RESULTS
Exposure to NM, either 1% or 2%, caused severe and long-lasting injury to ocular anterior segment structures. These findings were noted in previous reports and can be fully ap-preciated in the saline-treated, exposed eyes. The extent of injury was far more severe in eyes exposed to 2% NM: perfo-ration of the cornea occurred only after exposure to this higher concentration and only during the third or fourth week after injury. Four saline-treated eyes (4/8, 50%), as opposed to two Zn/DFO-treated eyes (2/8, 25%) and only one Ga/DFO-treated eye (1/8, 12.5%), perforated. Injury to the conjunctiva and cornea in a saline-treated eye that did not perforate after ex-posure to 2% NM is shown in Figure 1.
Conjunctival injury and scarring persisted for 4 weeks after exposure (Fig. 1A) and severe chronic corneal opacity and neovascularization were observed (Fig. 1B). Conjunctival and corneal injury was markedly reduced in eyes treated with Zn/DFO (group 2) and Ga/DFO (group 6), although some residual corneal opacity persisted (Fig. 1C, Ga/DFO treated eye). Histologic examination corroborated the clinical findings. As opposed to the normal corneal structure in the fellow uninjured eye (Fig. 1D), acanthosis, irregularities and some keratinization of the corneal epithelium, and infiltration of the corneal stroma by inflammatory cells, blood vessels, and hem-orrhages were seen in the eye exposed to 2% NM and treated by administration of saline only (Fig. 1E). Lysis of the extracel-lular matrix in the superficial stroma was also observed (Fig. 1E), which may explain the higher risk for corneal ulceration and perforation in such nontreated eyes. Corneal structure, as evident by histology, was much better preserved in Ga/DFO-and Zn/DFO-treated eyes (Fig. 1F, Ga/DFO). This protective effect could already be seen and quantified clinically during the early phases after injury and treatment: the corneal epithelial erosion caused by NM was similar in size in all experimental groups at day 1 after exposure, but was significantly reduced in Zn/DFO-treated eyes at day 3 (Table 2). Eyes treated with zinc (ZnCl2) or DFO alone did not significantly differ from saline-treated eyes at that time point.
Long-term visual outcome depends highly on the degree of corneal opacity that ultimately remains. On the first day after injury, during the acute phase, the average scores of corneal opacity were not statistically different among the groups (Fig. 2, left; each bar represents average of results in six eyes). However, the mean opacity score was significantly reduced 4 weeks after injury in the Zn/DFO- and DFO-treated eyes com-pared with saline-treated eyes (Fig. 2, right; P 0.05; each bar represents the average of results in six eyes, with each eye independently graded by four masked observers). For Zn/DFO, this represents 52% protection. Mean corneal opacity score in the Zn-treated eyes was also reduced, but this difference from saline-treated eyes was not statistically significant.
Exposure to NM also caused long-term changes in iris ap-pearance and structure. In the early postinjury period, dilation of iris vessels, iris stromal hemorrhages, and an inflammatory anterior chamber reaction were present. It was difficult, how-ever, to quantify these findings accurately behind the edema-tous and opaque cornea. As corneal condition stabilized (usu-ally within 7 to 14 days), it was possible to observe areas of iris pigmentation as well as atrophy in NM-exposed eyes (Fig. 3A) IOVS, July 2003, Vol. 44, No. 7
that were not present in noninjured fellow eyes (Fig. 3B). These changes were much less severe in NM-exposed eyes treated with Zn/DFO (Fig. 3C). The iris pigmentation score at 4 weeks after injury was significantly reduced (by 60%) in Zn/DFO-treated eyes compared with saline-treated eyes (Fig. 3D). Again, treatment with each component of the complex separately (i.e., ZnCl2 and DFO) showed a trend for reduction in severity that did not reach statistical significance (Fig. 3D; exemplified also in Fig. 4). To examine whether neovascular-ization of the iris occurred and whether vessel integrity was compromised after the acute injury phase, iris FA was per-formed at 4 to 5 weeks after exposure. As seen in Figure 4, the degree of pigmentation and atrophy differed between the treat-ment groups, but no leakage had occurred at that time. Histo-logic sections suggest that the pigmentation may be related to iris hemorrhages that occurred during the acute injury phase. Prussian blue staining showed hemosiderin in anterior segment structures of a 2% NM-exposed and saline-treated eye (Figs. 5A, 5C) that was not present in a nonexposed eye and was mark-edly reduced in a 2% NM-exposed and Ga/DFO-treated eye (Figs. 5B, 5D). We also observed evidence for thickening of the iris, loss of the natural posterior rugae, and formation of pos-terior synechia (adhesions) to the lens capsule in NM-exposed eyes treated with saline (Figs. 6D, 6E compared with Figs. 6A, 6B). Secondary cataractous lens changes occurred with the formation of morgagnian globules and lens epithelial necrosis (Figs. 6E, 6F). In Zn/DFO- and Ga/DFO-treated eyes, changes were much less severe (Figs. 6G–I).
As seen in Figure 7, IOP was elevated in all NM-injured eyes during the acute phase, peaking on day 4 after injury. The increase in IOP above nonexposed eyes was significantly re-duced (by 55%) in Zn/DFO- and Ga/DFO-treated compared with saline-treated eyes at this time point (P 0.05).
ERG that was performed in NM-injured, saline-treated eyes at 6 to 7 weeks after injury showed that retinal function was not affected by the anterior chemical injury: dark-adapted mixed rod– cone responses, rod responses, and light-adapted cone responses (at 1- and 30-Hz flicker) did not defer between NM-injured and fellow control eyes (results not shown). This is in accord with previous observations that posterior segment involvement in mustard-induced injury is rare.6 Treatment with Zn/DFO did not alter the ERG responses either, testifying to the safety of this complex (data not shown).
The level of oxidative stress associated with NM injury was assessed by measuring the dissipation of AA, an antioxidant and free radical scavenger, in systemic blood throughout the ex-periment. Even though only one eye (a relatively small organ) was affected, in saline-treated animals marked depletion of systemic AA occurred, supporting the role of free radical for-mation induced by exposure to NM (Fig. 8). AA levels were better preserved in eyes treated with Zn/DFO, indicating that the formation of free radicals was at least partially inhibited by this treatment. Ga/DFO had an identical effect.

DISCUSSION
Acute and chronic injury to anterior segment eye tissues after exposure to mustard agents is well documented in human subjects, as well as in animal models.5,7 To date, no specific effective treatment is available to reduce such ocular damage. Current regimens of treatment after ocular exposure to mus-tard chemicals are nonspecific and do not address the basic pathophysiology underlying the injury. Treatments include use of protective gear, removal of victims from contaminated areas, copious ocular irrigation, systemic analgesics in severe cases, application of mydriatic drugs to relieve ciliary muscle spasm and prevent formation of iris adhesions, antibiotic drops to IOVS, July 2003, Vol. 44, No. 7 Effective Treatment of Mustard Injuries 2971
FIGURE 7. IOP after exposure to 2% NM. IOP peaked at 4 days after in-jury, and from 1 week onward did not significantly differ from control, nonexposed eyes. Zn/DFO and Ga/ DFO significantly attenuated the in-crease in IOP at day 4, representing a 57% and 53% protective effect, re-spectively (inset; P 0.05, Mann-Whitney test). Each data point repre-sents mean IOP SEM in seven to eight eyes at days 0, 1, 4, 7, and 10 and mean IOP of four to eight eyes at days 14, 21, and 28.
prevent secondary bacterial infection, medications to control IOP, and use of lubricants.6 Some animal studies promote the topical use of corticosteroids and nonsteroidal anti-inflamma-tory drugs (diclofenac),18 colchicine,19 and a calcium-blocker (diltiazem)20 to reduce ocular inflammation. Reduced dermal and systemic injury, in animal models, was reported after treatment with thiosulfate, nicotinamide, flavonoids, and re-cently with topically applied iodine.6,21–24 However, no spe-cific antidote or highly effective treatment against mustard toxicity is currently available.
In the present study, we have demonstrated that topical application of low concentrations of Zn/DFO or Ga/DFO, after corneal exposure to NM, markedly reduced conjunctival, cor-neal, iris, and anterior chamber injury. In the cornea, faster healing of epithelial erosions, reduced long-term opacification and lower levels of neovascularization were observed. In the anterior chamber, decreased inflammation and better mainte-nance of IOP was achieved. Iris pigmentation and atrophy were not as severe, with less posterior adhesions of the iris to the lens. Cataractous changes were also notably milder.
It is assumed that NM injury, at least in part, is mediated by the formation of ROS, in addition to its action as an alkylating
FIGURE 8. Systemic oxidative stress as assessed by AA and its oxidized form, DHAA. OSAA [DHAA] 100/[AA] [DHAA]. From day 1 after exposure to 2% NM, markedly elevated levels of OSAA were observed in saline-treated animals, indicating high oxidative stress. In contrast, Zn/DFO- and Ga/DFO-treated animals demonstrated two- to sixfold lower levels. Difference is statistically significant at all time points (P 0.05, Mann-Whitney test). Each bar represents mean SEM of blood samples from four animals.
agent. Oxidative stress after ocular exposure to mustard has also been observed in other clinical studies7 and in animal models. Subcutaneous injection of a sulfur mustard analogue in mice increased the activity of several enzymes including glu-cose-6-phosphate dehydrogenase and glutathione S-trans-ferases.22 Dermally applied sulfur mustard caused systemic oxidative stress, raising the suggestion that flavonoids may help reduce toxicity.21 The marked depletion of systemic AA in the saline-treated group and the protective effect of Zn/DFO and Ga/DFO found in the present study lend further credence to this hypothesis.

We postulate that the protective effect of the complexes is the result of suppressed formation of ROS. The ability of these novel complexes to act through a combined push–pull mech-anism to achieve such a reduction in free radical formation is supported by both theoretical considerations and previously reported experimental findings. In the Fenton reaction or in the metal-mediated Haber-Weiss mechanism, the conversion of low reactive species to the highly reactive hydroxyl radicals apparently depends on the availability of trace amounts of the redox-active and labile iron or copper ions which serve as essential catalysts.11,25–27 It is hypothesized that either com-plex—Zn/DFO or Ga/DFO— exerts its protective effect by intervening in this critical step of hydroxyl radical formation. The two components of each of these complexes, when present at or near the site of injury, will ameliorate the avail-ability and catalytic activity of the redox-active metal ions through the push–pull mechanisms.12 In a number of experi-mental models, in which the formation of ROS plays a key role, Zn/DFO and Ga/DFO were indeed shown to afford marked protection against injury and inhibit the formation of free radicals. Thus, ischemia and reperfusion injury to the retina and heart were markedly reduced after systemic administration of either complex, as was the degree of corneal damage after topical use of Zn/DFO in alkali injury.12–15,28 Similarly, protec-
tion against the harmful effects of ionizing radiation was dem-onstrated.29,30The concern that mustard chemical warfare agents will be used in future terrorist acts or on the battlefield is quite real. In view of the marked protective effect observed in the present study, it is our opinion that the topical use of Zn/DFO or Ga/DFO should be considered as a basis for possible treatment of exposed human subjects. No ocular toxicity of the com-plexes themselves was observed. They were shown to be safe
2972 Banin et al.
when used systemically and topically in this and in other experimental models of ocular injury.13–15 It should be stressed, however, that treatment with the complexes did not completely ameliorate mustard-induced injury in our model. Moreover, follow-up in the present report was relatively short, whereas sequelae of mustard injury can continue for years. These are issues that require further study. Effectiveness may be improved by using a preparation that would allow increased residence time of the active complexes on the ocular surface. Such a preparation may also be useful in the treatment of exposed skin. In addition, preconditioning (initiating treat-ment shortly before potential exposure) may provide further benefit. Testing the efficacy of this treatment after exposure to sulfur mustard aerosol, rather than NM, is also a necessary step before this proposed treatment can be generally recom-mended.
In summary, our findings indicate clear advantages concur-rent with low toxicity of Zn/DFO and Ga/DFO in treatment of mustard injuries.
Acknowledgments
The authors thank Nahum Kittrosky and Israel Barzel for excellent technical assistance.
References
1. Blewett WK. Tactical weapons: is mustard still king? NBC Defence Technol Int. 1986;1:64 – 66.
2. Mohmad AH. Spatschaden der giftgaswirkung bei den Uberleb-enden des irakischen Giftgaskrieges gegen des kurdische volk.Wein Med Wochenscr. 1992;142:8 –15.
3. United Nations Security Council. Report of the Specialist Appoint-ment by the Security General to Investigate Allegations by the Islamic Republic of Iran Concerning the Use of Chemical Weap-ons. UN Report No. S/16433. New York: United Nations, 1986.
4. Pleyer U, Sherif Z, Baatz H, Hartman C. Delayed mustard gas keratopathy: clinical findings and confocal microscopy. Am J Oph-thalmol. 1999;128:506 –507.
5. Safarinejad MR, Moosavi SA, Montazeri B. ocular injuries caused by mustard gas: diagnosis, treatment, and medical defence. Mil Med. 2001;166:66 –70.
6. Solberg Y, Alcalay M, Belkin M. Ocular injury by mustard gas. Surv Ophthalmol. 1997;41:461– 466.
7. McGahan MC, Bito LZ. The pathophysiology of the ocular micro-environment. I. Preliminary report on the possible involvement of copper in ocular inflammation. Curr Eye Res. 1982;2:883– 885.
8. Kadar T, Turetz J, Fishbine E, Sahar R, Chapman S, Amir A. Char-acterization of acute and delayed ocular lesions induced by sulfur mustard in rabbits. Curr Eye Res. 2001;22:42–53.
9. Pfister RR, Haddox JL, Yuille-Bar D. The combined effect of citrate/ ascorbate treatment in alkali-injured rabbit eyes. Cornea. 1991;10: 100 –104.
10. Nirankari VS, Shambu DV, Lakhanpal V, Richards RD. Superoxide radical scavenging agents in treatment of alkali burns. Arch Oph-thalmol. 1981;99:886 – 887.
11. Chevion M. A site-specific mechanism for free radical induced biologic damage: the essential role of redox-active transition met-als. Free Radic Biol Med. 1988;5:26 –37. IOVS, July 2003, Vol. 44, No. 7
12. Chevion M. Protection against free radical-induced and transition metal-mediated damage: the use of “pull” and “push” mechanisms.
Free Radic Res Commun. 1991;12–13:691– 696.
13. Ophir A, Berenshtein E, Kitrossky N, Averbukh A. Protection of the transient ischemic cat retina by zinc-desferrioxamine. Invest Oph-thalmol Vis Sci. 1994;35:1212–1222.
14. Banin E, Berenshtein E, Kitrossky N, Pe’er J, Chevion M. Gallium-desferrioxamine protects the cat retina against injury after isch-emia and reperfusion. Free Radic Biol Med. 2000;28:315–323.
15. Siganos CS, Frucht-Pery J, Muallem MS, et al. Topical use of zinc desferrioxamine for corneal alkali injury in a rabbit model. Cornea. 1998;17:191–195.
16. Motchnik PA, Frei B, Ames BN. Measurement of antioxidants in human blood plasma. Methods Enzymol. 1994;234:269 –279.
17. Chevion S, Or R, Berry EM. The antioxidant status of patients subjected to total body irradiation. Biochem Mol Biol Int. 1999; 47:1019 –1027.
18. Amir A, Turetz J, Chapman S, Fishbeine E, et al. Beneficial effects of topical anti-inflammatory drugs against sulfur mustard-induced ocular lesions in rabbits. J Appl Toxicol. 2000;20 (suppl 1):S109 –S114.
19. Williams RN, Bhattacherjee P. Inhibition of the acute ocular re-sponses to nitrogen mustard by colchicines. Exp Eye Res. 1984; 39:721–729.
20. Gonzalez GG, Gallar J, Belmonte C. Influence of diltiazem on the ocular irritative response to nitrogen mustard. Exp Eye Res. 1995; 61:205–212.
21. Vijayaraghavan R, Sugendran K, Pant SC, et al. Dermal intoxication of mice with (2-chloroethyl) sulphide and the protective effect of flavonoids. Toxicology. 1991;69:35– 42.
22. Elsayed NM, Omaye ST, Klain Gj, et al. Free radical-mediated lung response to the monofunctional sulfur mustard butyl 2-chloroethyl sulfide after subcutaneous injection. Toxicology. 1992;72:153– 165.
23. Wormeser U, Sintov A, Brodsky B, Nyska A. Topical iodine prep-aration as therapy against sulfur mustard-induced skin lesions.
Toxicol Appl Pharmacol. 2000;169:33–39.
24. Wormser U, Brodsky B, Reich R. Topical treatment with povidone iodine reduces nitrogen mustard-induced skin collagenolytic activ-ity. Arch Toxicol. 2002;76:119 –121.
25. Chevion M, Jiang Y, Har-El R, Berenshtein E, Uretzky G, Kitrossky N. Copper and iron are mobilized following myocardial ischemia: possible criteria for tissue injury. Proc Natl Acad Sci USA. 1993; 90:1102–1106.
26. Liochev SI, Fridovich I. The Haber-Weiss cycle 70 years later: an alternative view. Redox Rep. 2002;7:55–57.
27. Stadtman E R. Protein oxidation in aging and age-related diseases. Ann N Y Acad Sci. 2001;928:22–38.
28. Karck M, Tanaka T, Berenshtein E, Haverich A, Chevion M. The push and pull mechanism to scavenge redox active transition metals: a novel concept in myocardial protection. J Thorac Car-diovasc Surg. 2001;121:1169 –1178.
29. Samuni Y, Coffin D, DeLuca AM, et al. The use of Zn-desferriox-amine for radioprotection in mice, tissue culture, and isolated DNA. Cancer Res. 1999;59:405– 409.
30. Nagler R, Marmary Y, Golan E, Chevion M. Novel protection strategy against X-ray-induced damage to salivary glands. Radiat Res. 1998;149:271–276.
